A_User
#63
Outcomes in RCT’s is way more important. A drug can target a genetic longevity pathway in a way that is harmful.
Neo
#64
Both sources of data in this situation seems to better than one only source (even if that source is better), if you were forced to only look at one source for some arbitrary reason.
Seems like an and and not an or case.
You can always take a low dose statin + Ezetemibe + Bempedoic Acid. The improvements are cumulative.
And for those of us who are intolerant to statins, Bempedoic Acid + Ezetemibe is our cost-effective solution.
1 Like
adssx
#66
I thought it was you @A_User who posted the paper saying that we needed a trial with something like 100k+ participants to be able to reach a conclusion on all cause mortality and that everything else was just noise?
Ezetimibe might have pro longevity effects in men btw: Higher LDL-Cholesterol is Associated with Greater Longevity? - #146 by adssx
And yes, bempedoic acid is so new, with so few RCTs, that it’s hard to conclude.
2 Likes
adssx
#67
Also: what’s the source? And is it an apple to apple comparison? Most trials of ezetimibe and bempedoic acid (alone or in combination) use these drugs in addition to statins or as first line therapy in statin-intolerant people. If we want to compare the effects on mortality of statins vs BA or EZE we need to look at RCTs that considered drug naive patients with dyslipidemia.
3 Likes
A_User
#68
JUPITER, among others for other statins, have detected decrease in ACM, so it is possible to have enough statistical power. If ACM has been detected, it is obviously superior as it explains risk vs. reward benefit (net benefit), and that there isn’t side effects which negate the benefits. There has at least been one statin that has been withdrawn from the market, and of course many other drugs.
So a drug that has detected ACM benefit is superior to one that hasn’t.
Even though a drug can target a longevity pathway, the effect depends on the molecule, so a drug can be harmful even though it targets a longevity pathway.
I don’t think any bempedoic acid trial have detected effects on mortality. If they haven’t studied BA in such a trial, that worsens the case for BA compared to statins?
L_H
#69
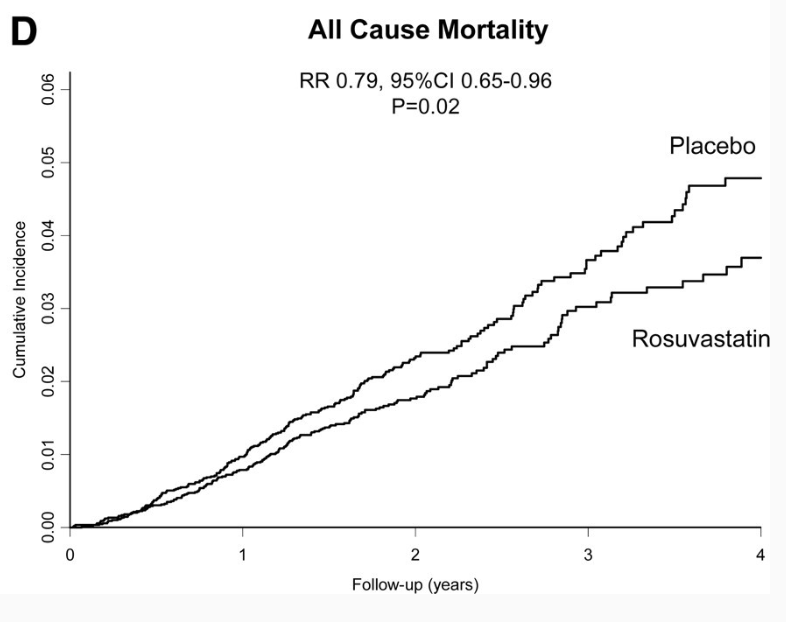
The Jupiter trial shows an ACM benefit from statins compared to placebo, but the data looks very odd. Im sure this has been covered to death. But its worth remembering that in the Jupiter trial the death rate of people taking statins was much higher than you’d expect in a similar match population of healthy individuals.
“The all-cause mortality in JUPITER was more than twice that of the average of primary prevention studies”
1 Like
We discussed some of the controversies in another thread. But just discussing ACM if I remember correct the authors were first publish this graph for ACM excluding some later data and were forced to retract it and change it:

The JUPITER trial is challenging to use as proof of statin primary prevention, as it did not demonstrate a reduction in ASCVD mortality. In my opinion, it was halted prematurely because it was becoming apparent that the net benefit of rosuvastatin was being offset by the increased incidence of new-onset diabetes cases in the rosuvastatin group, among other factors. Additionally, the ACM graph seemed to be showing convergence. Overall, JUPITER serves as a notable example of how statistics can be misleading and how financial interests can influence scientific outcomes.
2 Likes
KFISH
#71
Also may help more to reduce Lp(a) and trials suggests this effect on apoB.
A_User
#72
What retraction? Can you link?
Where did you see that it did not reduce ASCVD mortality?
At the end of the graph, the difference between placebo and rosuvastatin was pretty much greater than at other points in the graph, excluding the period about 3.3-4 years into the study were there were a greater difference. You can also look through the entire graph and see a dozen convergences.
sample size was about 17+k
CV mortality
placebo: 37 events
MI 6 events
Stroke 6 events
other CV death 25 events
rosvustatin: 31 events
MI 9 events
Stroke 3 events
other CV death 19 events
A_User
#74
All-cause mortality is a more precise measurement, so it doesn’t matter (for example, deaths might be misreported as not CVD related).
adssx
#75
Yes.
Yes. But here we have pathway (MR) + animal study + RCT in humans hinting at potential longevity effects in men. It’s just a “hint”. TBC.
I agree that the case for BA is not extremely strong (due to the low number of studies), except in statin-intolerant people (and maybe in people with T2D). I was interested in BA, but the +14.8% increase in serum uric acid levels is concerning to me:
-
Efficacy and safety of bempedoic acid lipid-lowering therapy: a systematic review and meta-analysis of randomized controlled trials 2023: “There was a significant reduction in the risk of MACE [RR, 0.88 (95% CI: 0.77 to 0.99), p = 0.03)] and all-cause mortality [RR, 0.90 (95% CI: 0.82 to 0.98), p = 0.02] following bempedoic acid treatment. […] However, there was a significant increase in the risk of hyperuricemia [RR, 2.05 (95% CI: 1.81 to 2.33), p < 0.001] following bempedoic acid treatment.”
-
Effect of bempedoic acid on uric acid and gout in 3621 patients with hypercholesterolemia: pooled analyses from phase 3 trials 2020: “At week 12, mean (SD) serum uric acid levels (% change from baseline) increased from baseline with BA treatment by 0.82 (0.97) mg/dL (14.8%) vs –0.02 (0.82) mg/dL (0.67%) for placebo. Elevations in serum uric acid levels typically occurred within the first 4 weeks of treatment, remained stable during treatment, and returned to baseline after treatment discontinuation. Gout was reported in 1.4% (BA) and 0.4% (placebo) of patients, and hyperuricemia was reported in 1.7% (BA) and 0.6% (placebo) of patients.”
1 Like
A_User
#76
That’s good, so there is probably a net benefit. But it is a meta analysis, and that is worse than a large RCT detecting ACM benefit.
adssx
#77
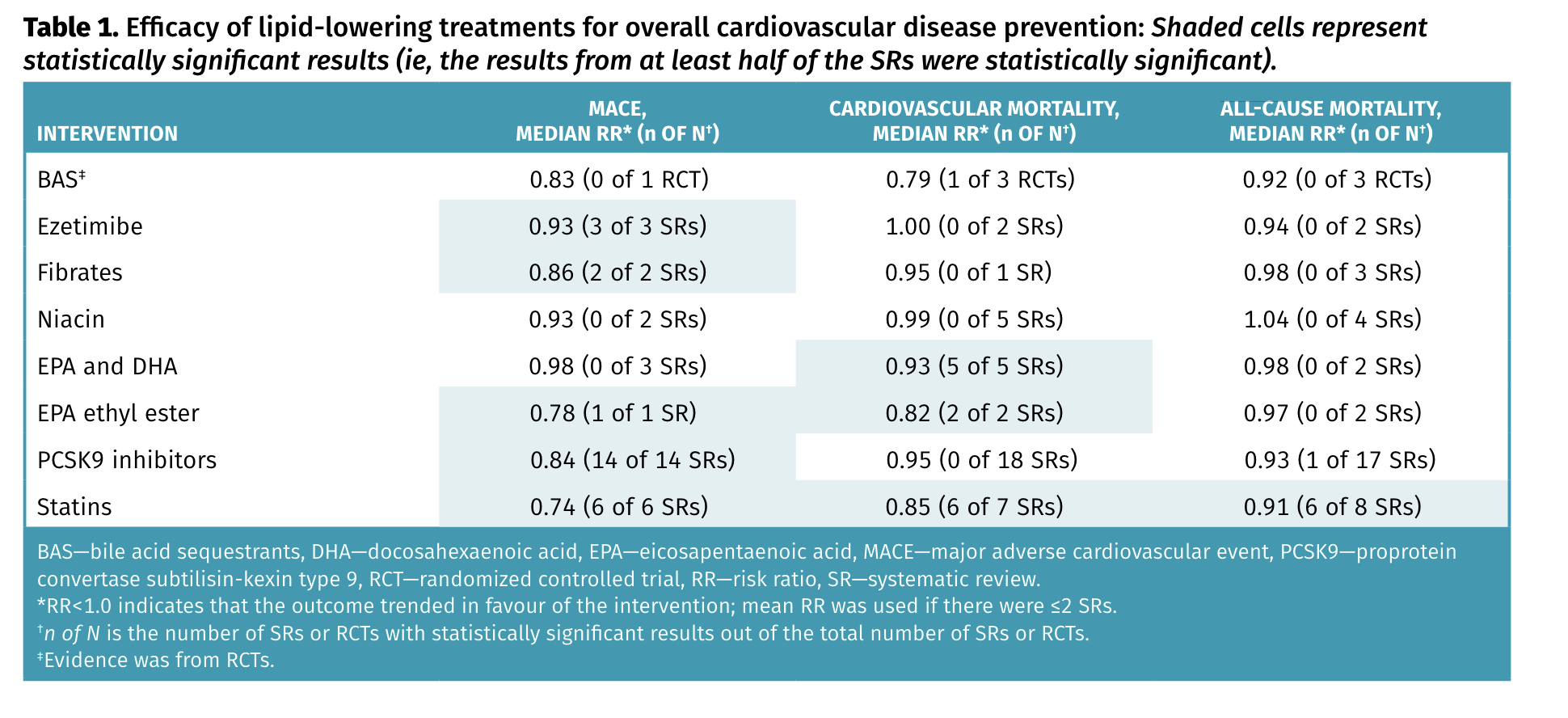
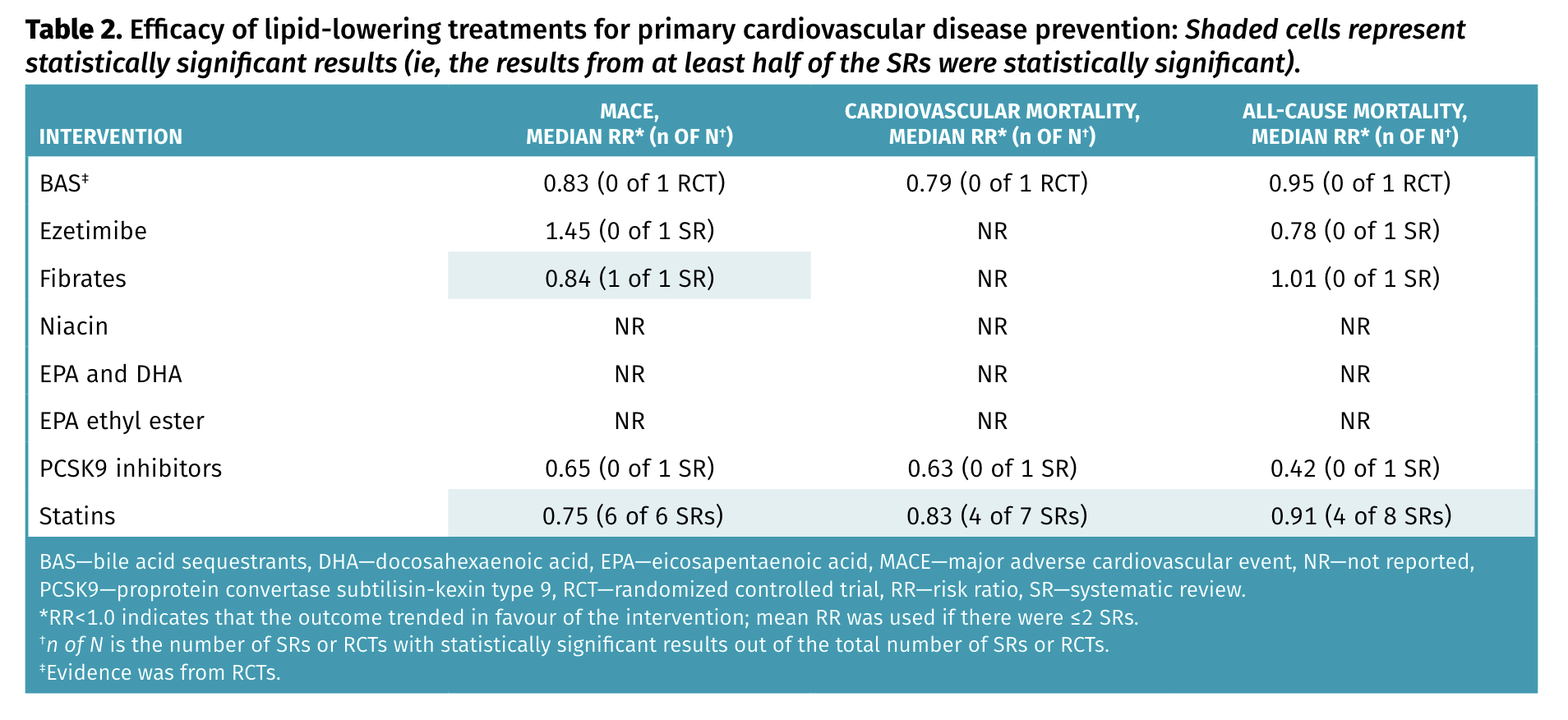
I disagree, but it’s OK because here’s a recent review that confirms your point on statins’ benefits: Lipid-lowering therapies for cardiovascular disease prevention and management in primary care PEER umbrella systematic review of systematic reviews 2023 ( Bempedoic acid was not analyzed as part of the review )
Bempedoic acid was not analyzed as part of the review )
Statins remain the lipid-lowering drugs with the most consistent benefits, with a relative risk reduction of approximately 25% for major adverse cardiovascular events (MACE) and approximately 10% for mortality. Although MACE was also reduced with ezetimibe (about 7% relative), fibrates (about 15% relative), and proprotein convertase subtilisin-kexin type 9 inhibitors (about 15% relative), these drugs had no effect on cardiovascular mortality or all-cause mortality.
(still, in primary prevention, ezetimibe and PCSK9 seem interesting, TBC. I’d like to see results stratified by gender as well)
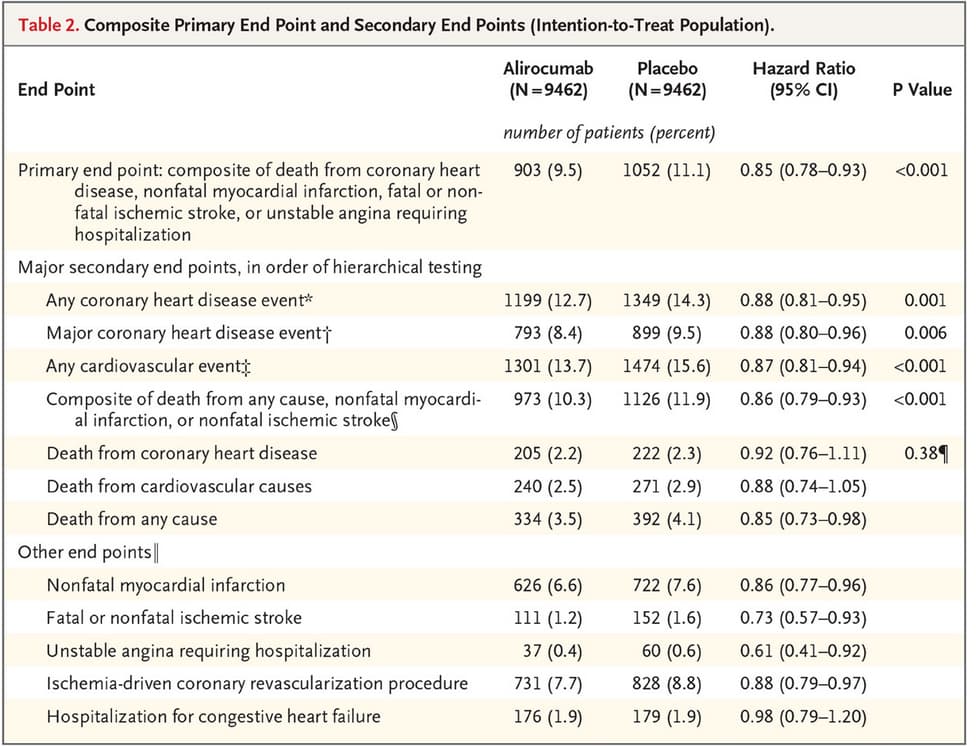
In PCSK9i, alirocumab but not evolocumab reduces ACM (and by a lot more than statins: 0.6 OR!): PCSK9 inhibitors and small interfering RNA therapy for cardiovascular risk reduction: a systematic review and meta-analysis 2023
After a median of 26 months, Evolocumab reduced the risk of myocardial infarction (MI), OR 0.72 (95% CI: 0.64, 0.81, p<0.01), coronary revascularization, OR 0.77 (95% CI: 0.70, 0.84, p<0.01), stroke, OR 0.79 (95% CI: 0.66, 0.94, p = 0.01) and overall MACE, OR 0.85 (95% CI: 0.80, 0.89, p<0.01). Alirocumab reduced MI, OR 0.57 (0.38, 0.86, p = 0.01), cardiovascular mortality OR 0.35 (95% CI: 0.16, 0.77, p = 0.01), all-cause mortality OR 0.60 (95% CI: 0.43, 0.84, p<0.01), and overall MACE OR 0.35 (0.16, 0.77, p = 0.01). Insufficient MACE data has been reported for Inclisiran.
(@Neo: which one are you taking?)
This shows that concluding about one class can be irrelevant. We shouldn’t necessarily look at all statins but at the best in class (rosuvastatin?).
Also, lipid-lowering therapies might shift mortality from CVD to cancer in people >75yo: Is there a shift from cardiovascular to cancer death in lipid-lowering trials? A systematic review and meta-analysis 2024
1 Like
A_User
#78
Yes it’s not enough to to only look at mechanism of action (i.e reducing apoB), but also class of drugs and outcomes (i.e statins) and best in class (maybe rosuvastatin). Ultimately the comparison is between different drugs. Like alirocumab vs. rosuvastatin, or even a combination, like for reducing apoB further, basically the question is what is the best way to reduce apoB? I would still place higher value on drugs detecting effects in large RCT’s compared to systematic reviews summating different values.
Although the data for ACM in the Alirocumab trial was good, they didn’t calculate because they ran into a non-stat sig result before it, which still makes for example rosuvastatin slightly better IMO.
L_H
#79
Yes the Jupiter data is surprisingly weak, considering they stopped it. Do you know when the staree trial is due to report?
https://www.monash.edu/medicine/staree/home
Neo
#80
Evolocumab / Repatha. Think the liver risks were smaller.
Was considering a potential shift to Alirocumab / Prauluent recently after some weird Lp(a) numbers and when seeing a cost difference emerge in Praulents favor.
Above makes me want to look into that further. Thank you for sharing.
2 Likes
Neo
#81
I don’t belive that is correct. What those facts tell us is that it might be better. But it might not.
You heave more certainty for the one that showed the effect, and you have more uncertainty for the second one, but that does not mean that the second one (if its trials were too short and too small for all cause statistical power) has a negative signal - rather it means that we don’t know.
And that is where all the other triangulation should come in.
For instance, was all cause mortality reduction of statins similar for women and men in the statins case? If you don’t know, as a male you might want to look into that if you have a choice between statin and other options for Abo B lowering - as the impact of poor metabolic health and diabetes risks seems worse for male longevity than in women - might be relevant as in statins case metabolic health / glucose control / diabetes are known side effect risks.
Similarly, the cancer point that was raised above (though in older patients), to the extent that is mediated via impairments in metabolic health/glucose control from stations, might be a larger risk for men than women.
What is your risk profile as it pertains to dementia, diabetes, cancer vs other things?
Are you a cholesterol over producer or over absorber? @A_User do you knot agree that knowledge can be very valuable in deciding on Apo B lowering med(s)?
What does your other blood work tell you and how does that other bloodwork change when you try a given Apo B medicine?
2 Likes
Neo
#82
What have people taking Bemp Acid here experienced such changed? @DeStrider ?
1 Like