I disagree, but it’s OK because here’s a recent review that confirms your point on statins’ benefits: Lipid-lowering therapies for cardiovascular disease prevention and management in primary care PEER umbrella systematic review of systematic reviews 2023 ( Bempedoic acid was not analyzed as part of the review )
Bempedoic acid was not analyzed as part of the review )
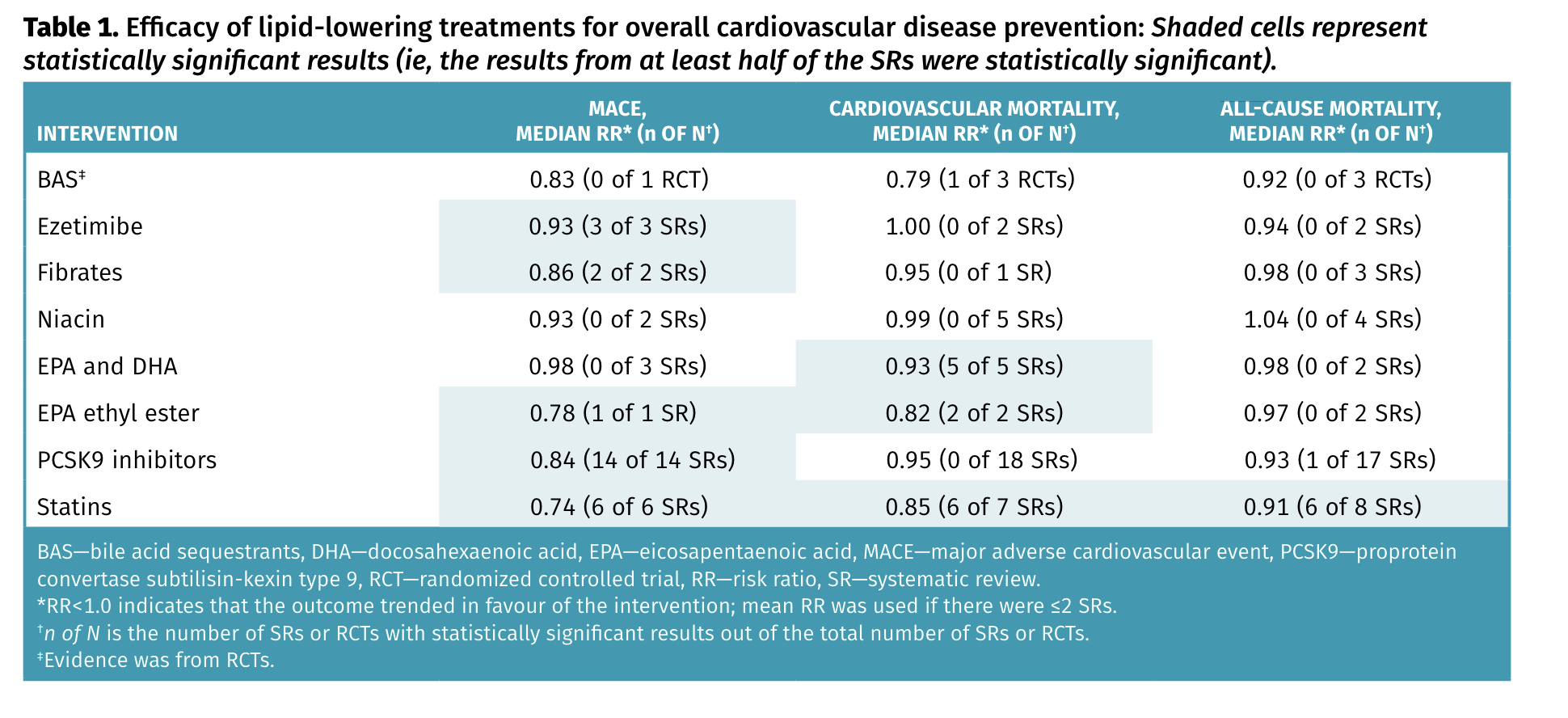
Statins remain the lipid-lowering drugs with the most consistent benefits, with a relative risk reduction of approximately 25% for major adverse cardiovascular events (MACE) and approximately 10% for mortality. Although MACE was also reduced with ezetimibe (about 7% relative), fibrates (about 15% relative), and proprotein convertase subtilisin-kexin type 9 inhibitors (about 15% relative), these drugs had no effect on cardiovascular mortality or all-cause mortality.
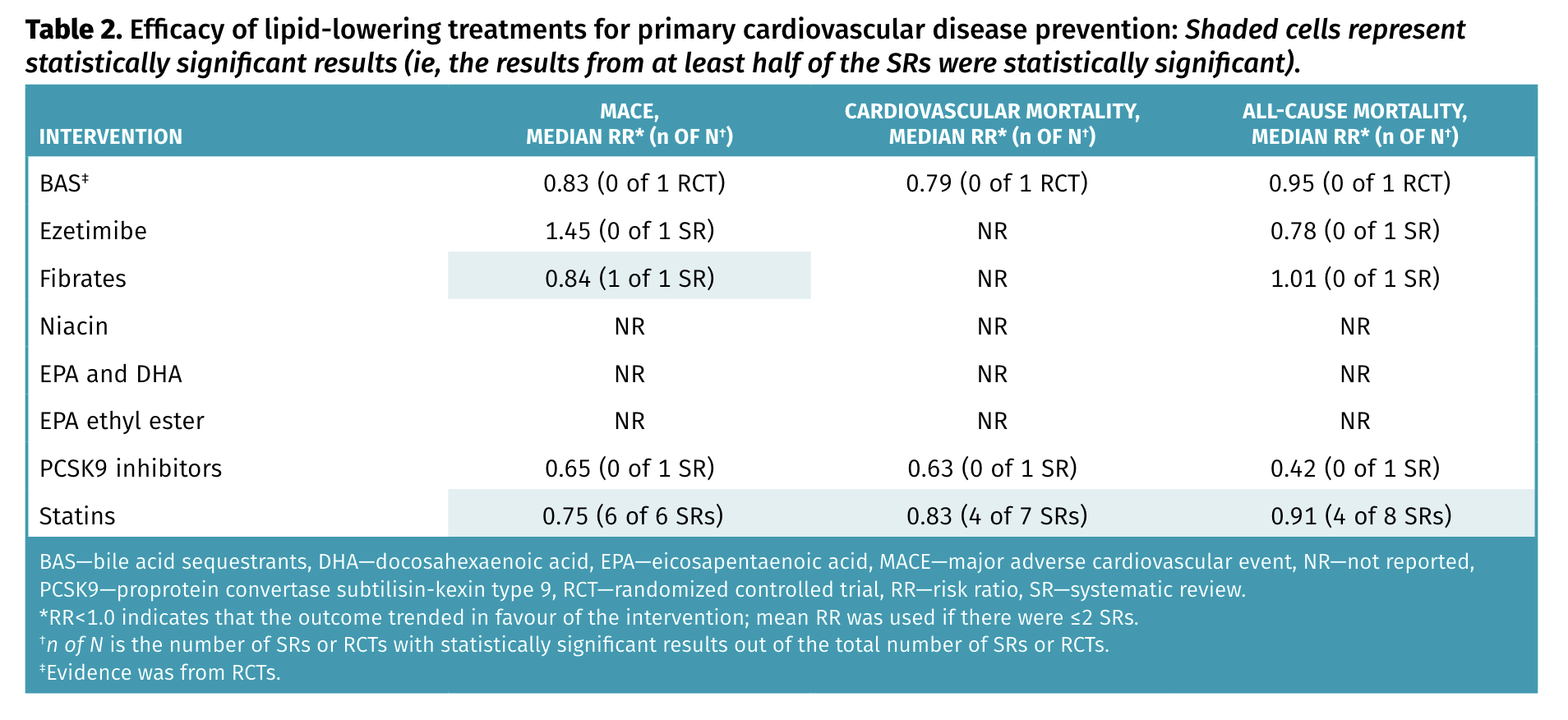
(still, in primary prevention, ezetimibe and PCSK9 seem interesting, TBC. I’d like to see results stratified by gender as well)
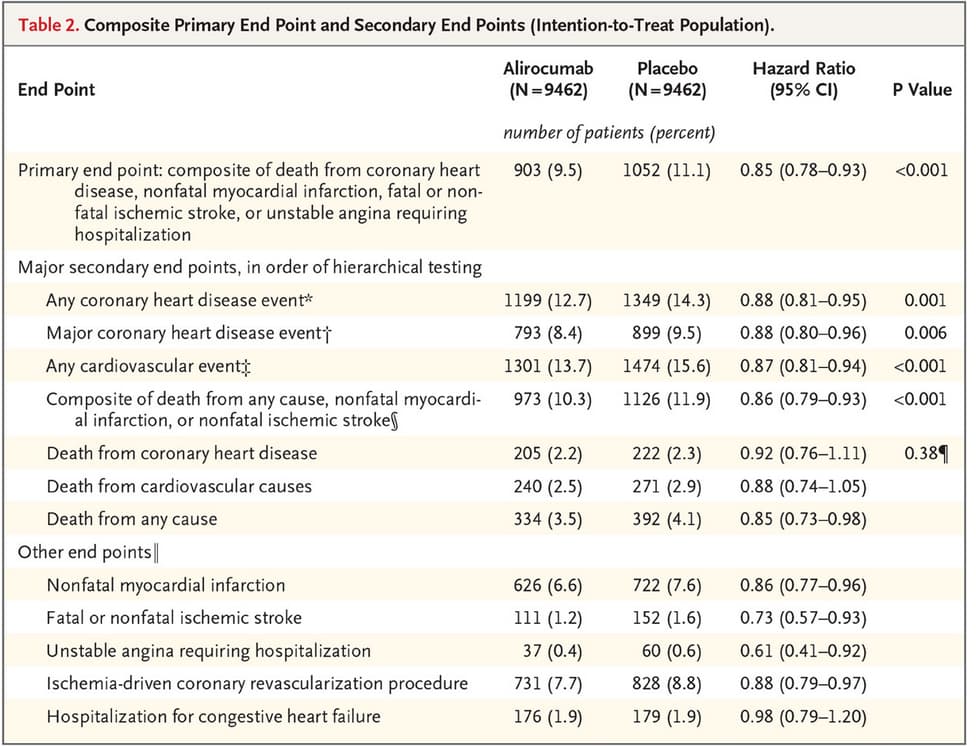
In PCSK9i, alirocumab but not evolocumab reduces ACM (and by a lot more than statins: 0.6 OR!): PCSK9 inhibitors and small interfering RNA therapy for cardiovascular risk reduction: a systematic review and meta-analysis 2023
After a median of 26 months, Evolocumab reduced the risk of myocardial infarction (MI), OR 0.72 (95% CI: 0.64, 0.81, p<0.01), coronary revascularization, OR 0.77 (95% CI: 0.70, 0.84, p<0.01), stroke, OR 0.79 (95% CI: 0.66, 0.94, p = 0.01) and overall MACE, OR 0.85 (95% CI: 0.80, 0.89, p<0.01). Alirocumab reduced MI, OR 0.57 (0.38, 0.86, p = 0.01), cardiovascular mortality OR 0.35 (95% CI: 0.16, 0.77, p = 0.01), all-cause mortality OR 0.60 (95% CI: 0.43, 0.84, p<0.01), and overall MACE OR 0.35 (0.16, 0.77, p = 0.01). Insufficient MACE data has been reported for Inclisiran.
(@Neo: which one are you taking?)
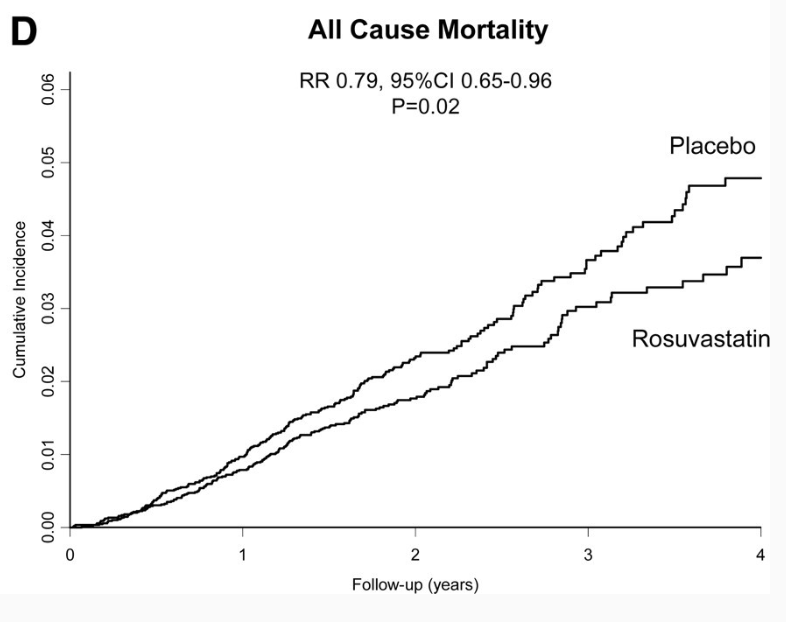
This shows that concluding about one class can be irrelevant. We shouldn’t necessarily look at all statins but at the best in class (rosuvastatin?).
Also, lipid-lowering therapies might shift mortality from CVD to cancer in people >75yo: Is there a shift from cardiovascular to cancer death in lipid-lowering trials? A systematic review and meta-analysis 2024