Do you need to drop it below 50? Atherosclerosis is a function of both time and ApoB levels. Unless there is some compelling reason to go below 50 soon, it seems the stats tell us that below 70 is good enough for many decades. Again unless there are other reasons, such as a lot of plaque, obstructions and stenosis in the vasculature, high blood pressure, very low HDL levels, high Lp(a), high inflammation as scored by hsCRP above 1.5 or so, uncontrolled diabetes, diagnosed CHD, CAD or HF, dire family history, current smoker, etc. Without significant risk factors I would not worry about going below 50 if I were 80yo, in fact I’m 66, and would be happy as long as I’m not above 70. The additional 30 point drop doesn’t buy you much compared to the possible risks or side effects of multiple medications needed to achieve that 30 point drop. I would vote to relax and not worry if the number is not much below 70. But, I’m not a doctor, and I don’t know your exact situation.
1 Like
mccoy
#22
I am experimenting minidoses of rosuvastatin (other statins would do) + minidoses of ezetimibe. This after the extensive references posted in this forum.
1/4 the minimal dose commercially available is what I’d call an actionable minidose (the circular pill can be divided in 4ths, the oval pill as well, although with more effort.
In your case, you might add a daily minidose of crestor for example (1/4 of a 4 mg pill), which would probably avoid side effects.
For oval piplls a minidose can be achieved by halving the pill and taking it every other day. It equals 1/4 he original intended amount.
4 Likes
A_User
#23
Where does the side effects from increased dosing come from? Do anyone know?
If I’m to speculate, at a certain dosage you have maximum HMGCR inhibition in the liver. Past this threshold there are diminishing returns on inhibition in the liver and there are more of the statin systemically leading for example to very rarely a decrease in glucose sink in the muscles.
nikney
#24
The half-life of ezetimibe is 22 hours, which is relatively long. Is there anyone who uses ezetimibe in intermittent dosage form? For example, 3 days a week?
1 Like
RobTuck
#25
Thanks for all of the suggestions. They caused me to go back to the data where I see that I am jumping the guns as mentioned. Most of the large studies that examined Apo(b) in relation to significant ASCVD events fail to show improvement or de minimus improvement below Apo(b) of 70 or 80. One large study saw small but significant additional benefit all the way down to 60. Combining that information with the fact that at my age my arteries are what they are and the most reasonable goal is to minimize additional harm, I think achieving a level of 70 is an aggressive personal goal. As I have mentioned, my overarching goal remains keeping inflammation at its lowest possible levels so as not to precipitate an event. Past 70 or so, this goal seems to have the most leverage on overall health.
3 Likes
mccoy
#26
I think there are quite a few people, including myself. I’m taking 2.5 mg ezetimibe every other day, with a daily average of 1.25 mg.
1 Like
RobTuck
#27
What is your reason for taking a lower dose?
mccoy
#28
My reason is that I want to try and increase the intake of saturated fats (more calories) while decreasing a little the blood lipid values, which are not bad currently. I’m going to check this strategy soon.
RobTuck
#29
Understood. Good luck @mccoy. My LDL and Apo(b) were out of bounds so BP and EZ constitute the pharmaceutical portion of my effort to bring them down. Diet and lifestyle can bring both into line if you are not too far off of your goal but I was unable to get either where I wanted them with excellent diet and a vigorous and balanced exercise program. In addition, I didn’t feel good on the diet that lowered these metrics the most even though my B-12 and related metrics were good. It was difficult for me to eat enough to get enough protein to support my weight lifting and hiking activities. I was forcing food down and my muscles were wasting. I have added judicious amounts of meats back into my diet. I feel good again and my muscle development has done a 180.
2 Likes
RobTuck
#30
JAMA: Bempedoic Acid for Primary Prevention of Cardiovascular Events in Statin-Intolerant Patients
jama_nissen_2023_oi_230067_1688654420.59513.pdf (504.6 KB)
3 Likes
mccoy
#32
The above, although anecdotal, is representative of the variability of individual response in diet and lifestyle. I too had a similar catabolic response to a low-carb regime, and turned back to normal. Priorities (decent muscularity) are priorities, LOL
2 Likes
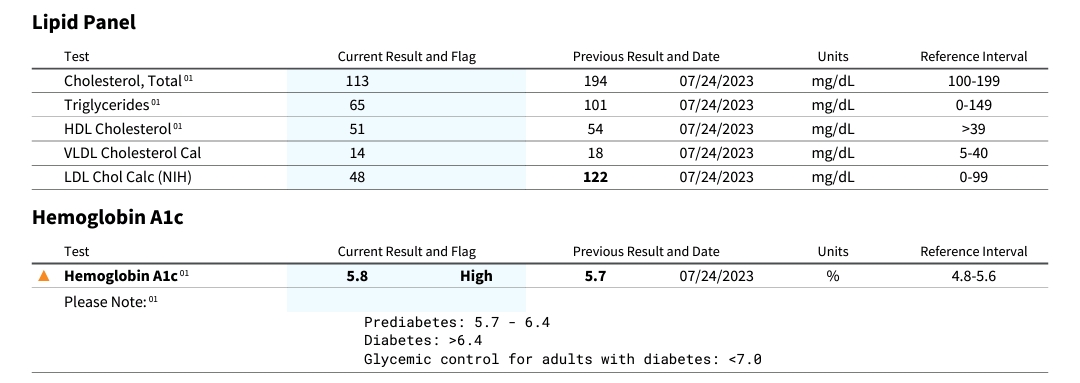
Updated results for me. I added 5 mg of daily Lipitor (Atorvastatin) before this test last summer. HBA1C is back to a problem range. 
3 Likes
mccoy
#34
I would rather say that, considering the measurement error and the natural fluctuations in a biologic parameter, even if that’s a time-average, your HBA1C is basically the same as before.
4 Likes